Photo by Dr. Frederick A. Murphy
You call a friend and arrange to meet for lunch. It’s unseasonably springlike, so you choose a place with outdoor seating, which seems like it should be safer. As usual, you take all reasonable precautions: You use hand sanitizer, sit a good distance from other customers, and try to avoid touching your face, though that last part is hard. A part of you suspects that this whole thing might be overblown.
What you don’t know is that ten days ago, your friend’s father was a guest of his business partner at the University Club, where he caught the novel coronavirus from the wife of a cryptocurrency speculator. Three days after that, he coughed into his hand before opening the door of his apartment to welcome his son home. The saliva of COVID-19 patients can harbor half a trillion virus particles per teaspoon, and a cough aerosolizes it into a diffuse mist. As your friend walked through the door he took a breath and 32,456 virus particles settled onto the lining of his mouth and throat.
Viruses have been multiplying inside his body ever since. And as he talks, the passage of his breath over the moist lining of his upper throat creates tiny droplets of virus-laden mucus that waft invisibly into the air over your table. Some settle on the as-yet-uneaten food on your plate, some drift onto your fingers, others are drawn into your nasal sinus or settle into your throat. By the time you extend your hand to shake good-bye, your body is carrying 43,654 virus particles. By the time you’re done shaking hands, that number is up to 312,405.
Read more of this here: New York Magazine: How the Coronavirus Could Take Over Your Body (Before You Ever Feel It) by Jeff Wise, 3/18/2020.
1/14/2021 The Coronavirus Is Mutating. Here’s What We Know, Wall Street Journal Video
1/12/2021 The Future of the Coronavirus? An Annoying Childhood Infection, by Apoorva Mandavilli, The New York Times
As millions are inoculated against the coronavirus, and the pandemic’s end finally seems to glimmer into view, scientists are envisioning what a postvaccine world might look like — and what they see is comforting.
The coronavirus is here to stay, but once most adults are immune — following natural infection or vaccination — the virus will be no more of a threat than the common cold, according to a study published in the journal Science on Tuesday and reported in the New York Times.
12/28/2021 The Science Behind How the Coronavirus Affects the Brain, WSJ Video
New research could help explain why thousands of Covid-19 survivors are facing debilitating neurological symptoms months after initially getting sick.
12/10/2020 Genomic Vaccines Fight Disease in Ways Not Possible Before. Rudy Giuliani was allocated one of the only 108 doses distributed to Washington D.C.
11/18/2020 How Doctors Can Predict Who Dies From COVID, Mike Hansen MD (a 7 minute youtube tutorial)
Mortality was 28.8% in the group that met criteria, vs 6.6% in those who did not meet criteria. So if they met cytokine storm criteria, their likelihood of dying was 4 times higher. And how accurate was this prediction model? Pretty accurate, as this study had a specificity of 79% and a sensitivity of 85%, which is a lot of predictive power.
11/9/2020 How the Coronavirus Hacks the Immune System, by James Somers, The New Yorker
At a laboratory in Manhattan, researchers have discovered how SARS-CoV-2 uses our defenses against us. TenOever’s team quickly discovered that sars-CoV-2 was uncannily good at disrupting cellular programming. A typical virus replaces less than one per cent of the software in the cells it infects. With sars-CoV-2, tenOever said, about sixty per cent of the RNA in an infected cell is of viral origin—“which is the highest I’ve ever seen. Polio comes close.” Among other things, the virus rewires the alarm system that cells use to warn others about infection.
11/5/2020: Clots, Strokes And Rashes. Is COVID-19 A Disease Of The Blood Vessels? by Will Stone, NPR
Some of the earliest insights into how COVID-19 can act like a vascular disease came from studying the aftermath of the most serious infections. Those reveal that the virus warps a critical piece of our vascular infrastructure: the single layer of cells lining the inside of every blood vessel, known as the endothelial cells or simply the endothelium.
Dr. William Li, a vascular biologist, compares this lining to a freshly resurfaced ice skating rink before a hockey game on which the players and pucks glide smoothly along.
"When the virus damages the inside of the blood vessel and shreds the lining, that's like the ice after a hockey game," says Li, a researcher and founder of the Angiogenesis Foundation. "You wind up with a situation that is really untenable for blood flow."
9/18/2020 Stroke patients with COVID-19 experience more severe symptoms, a much higher mortality rate, by Michael Walter, Cardiovascular Business
While the study did only focus on a limited number of patients, the authors also noted that the mortality rate was 44.4% for stroke patients with COVID-19 compared to 7.6% for those without COVID-19. For discharged patients, the average length of hospital stay was also longer if the patient had COVID-19.
8/13/2020: Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a population-based cohort study, by Naomi Holman, PhD, Peter Knighton, MPhys, Prof Partha Kar, MD, Jackie O'Keefe, MSc, Matt Curley, BA, Andy Weaver, MSc, et al., The Lancet
Diabetes has been associated with increased COVID-19-related mortality, but the association between modifiable risk factors, including hyperglycaemia and obesity, and COVID-19-related mortality among people with diabetes is unclear. We assessed associations between risk factors and COVID-19-related mortality in people with type 1 and type 2 diabetes.
8/11/2020 Why the Heart Attack Death Rate Has Doubled During COVID-19, by Brian Krans, Healthline
5/29/2020: Medium: Coronavirus May Be a Blood Vessel Disease, Which Explains Everything, by Dana G. Smith
“It turns out that both statins and ACE inhibitors are extremely protective on vascular dysfunction,” Mehra says. “Most of their benefit in the continuum of cardiovascular illness — be it high blood pressure, be it stroke, be it heart attack, be it arrhythmia, be it heart failure — in any situation the mechanism by which they protect the cardiovascular system starts with their ability to stabilize the endothelial cells.”
Mehra continues, “What we’re saying is that maybe the best antiviral therapy is not actually an antiviral therapy. The best therapy might actually be a drug that stabilizes the vascular endothelial. We’re building a drastically different concept.”
5/21/2020: NEJM: Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19, by Maximilian Ackermann, M.D., Stijn E. Verleden, Ph.D., Mark Kuehnel, Ph.D., Axel Haverich, M.D., Tobias Welte, M.D., Florian Laenger, M.D., Arno Vanstapel, Ph.D., Christopher Werlein, M.D., Helge Stark, Ph.D., Alexandar Tzankov, M.D., William W. Li, M.D., Vincent W. Li, M.D., et al.m
The lungs from patients with Covid-19 also showed distinctive vascular features, consisting of severe endothelial injury associated with the presence of intracellular virus and disrupted cell membranes. Histologic analysis of pulmonary vessels in patients with Covid-19 showed widespread thrombosis with microangiopathy. Alveolar capillary microthrombi were 9 times as prevalent in patients with Covid-19 as in patients with influenza (P<0.001). In lungs from patients with Covid-19, the amount of new vessel growth — predominantly through a mechanism of intussusceptive angiogenesis — was 2.7 times as high as that in the lungs from patients with influenza (P<0.001).
5/18/2020: Medium: Every Covid-19 Symptom We Know About Right Now, From Head to Toe, by Robert Roy Britt
5/4/2020 Why Lying Face-Down Helps Relieve Coronavirus Symptoms, by Jesse Smith, 5/4/2020
How 'proning' Covid-19 patients helps them breathe
How Covid-19 Immunity Compares to Other Diseases
4/28/2020 COVID-19: What the data shows, Heart & Stroke
4/24/2020: Daily Beast: How the Coronavirus Sneaks into Your Body, A Rabbit Hole Deep Dive
In order to find which cells might be the gateways for the virus, Cambridge researchers turned to the Human Cell Atlas. The atlas, launched in 2016, acts as a kind of map for the hundreds of different kinds of cells in your body, their characteristics, the genes they contain, and their relationship to other cells.
The coronavirus works by attaching its spike protein to a particular receptor on the outside of human cells referred to as ACE2 and a protein in cell membranes named TMPRSS2 which primes those receptors for the virus to enter. The cells with the highest levels of ACE2 and TMPRSS2 turned out to be in the nose — goblet cells that make mucus and ciliated cells, tiny cells that look like miniature wheat fields which clean stray bits of snot and foreign organisms out of your airways.
While the highest levels of ACE2 and TMPRSS2 were found in cells in the nose, the Cambridge team also found high levels in cells associated with other organs. Cells in the human cornea and intestines also had plenty of the coronavirus-friendly proteins
At the outset of the pandemic, a pneumonia specialist in China became infected after inspecting a hospital while wearing an N95 mask and no eye protection and developed conjunctivitis shortly before becoming symptomatic.
4/23/2020: Nature Medicine: SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes, by Waradon Sungnak, Ni Huang, Christophe Bécavin, Marijn Berg, Rachel Queen, Monika Litvinukova, Carlos Talavera-López, Henrike Maatz, Daniel Reichart, Fotios Sampaziotis, Kaylee B. Worlock, Masahiro Yoshida, Josephine L. Barnes & HCA Lung Biological Network
We investigated SARS-CoV-2 potential tropism by surveying expression of viral entry-associated genes in single-cell RNA-sequencing data from multiple tissues from healthy human donors. We co-detected these transcripts in specific respiratory, corneal and intestinal epithelial cells, potentially explaining the high efficiency of SARS-CoV-2 transmission.
We provide our data in a comprehensive, open and user-friendly fashion at www.covid19cellatlas.org
4/20/2020: The Lancet: Endothelial cell infection and endotheliitis in COVID-19, by Zsuzsanna Varga, Andreas J Flammer, Peter Steifer, Martina Haberecker, Rea Andermatt, Annelies S. Zinkernagel, et al
4/17/2020: Science: How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes, by Meredith Wadman, Jennifer Couzin-Frankel, Jocelyn Kaiser, Catherine Matacic
How the virus attacks the heart and blood vessels is a mystery, but dozens of preprints and papers attest that such damage is common. A 25 March paper in JAMA Cardiology documented heart damage in nearly 20% of patients out of 416 hospitalized for COVID-19 in Wuhan, China. In another Wuhan study, 44% of 36 patients admitted to the ICU had arrhythmias.
The disruption seems to extend to the blood itself. Among 184 COVID-19 patients in a Dutch ICU, 38% had blood that clotted abnormally, and almost one-third already had clots, according to a 10 April paper in Thrombosis Research. Blood clots can break apart and land in the lungs, blocking vital arteries—a condition known as pulmonary embolism, which has reportedly killed COVID-19 patients. Clots from arteries can also lodge in the brain, causing stroke. Many patients have “dramatically” high levels of D-dimer, a byproduct of blood clots
4/11/2020: The Mercury News: When coronavirus kills, it’s like death by drowning — and doctors disagree on best treatment, by Lisa M. Krieger
In a comparison of very sick patients in China, shortness of breath began around the seventh day of their illness, with sepsis starting on the ninth or 10th day, followed by ARDS and then ICU admission on the 12th day, said Babik. The heart and kidneys showed injury on the 15th day. On the 17th day, secondary infections began to set in. Patients died, on average, on the 19th day.
Most worrisome: As the disease progresses, ventilators aren’t saving people. Despite our best efforts, COVID-19 illness is far more lethal than traditional ARDS, claiming not 40% of victims but 70% or even 80%.
Twitter: I don’t usually rant on social media. However, after a week of service in the ICU, I’d like to get a few things off my chest. #COVID19 (1/10) by Sanjum S. Sethi MD, MPH Click here to access the Twitter thread
1) This is a horrible, relentless, nasty disease in its severe form. If the patient is obese and/or has renal failure, the prognosis is extremely grim. They are NOT dying from comorbidities. They are dying from COVID -19.
2) When I say relentless; most patients make some improvements initially (days 4-6), but decompensate with a 2nd cytokine storm (as many have described). It is this 2nd decompensation that is deadly and that we need to prevent.
3) We are forced to share dialysis circuits given the high percentage of renal failure (these people had normal kidneys before!) Why isn’t there more press for this fact? We need more machines to manage our patients effectively.
4) This IS ARDS full stop. While certain pts may be phenotypically different and benefit from lower PEEP, others de recruit quickly. Different phenotypes should be treated as such. We are seeing more atypical presentations than usual because the volume is tremendous.
5) My interest is in thrombosis and there is a definite hypercoagulable state associated with this illness. Anticoagulation is all over the place at different centers, but there is no randomized data yet to guide any of it (working on it).
6) Every single ICU patient (barring QTc issues) got hydroxychloroquine and it doesn’t seem to have helped. Maybe it helps for prophylaxis or in mild disease, but doesn’t appear to do anything once in ICU. It is NOT a pancea and should not be given indiscriminately.
7) Listen to people who have been studying viruses and ARDS before all this began and will continue to investigate/clinically deal with it long after we have all moved on. #COVID19 #DrFauci
8) Be skeptical, but armchair conspiracy theories without any viable solutions are extremely disheartening. We are all in this together, help us generate the data that will answer those questions you are skeptical about and more importantly help our patients.
9) The rapid dissemination of materials, protocols, data is truly impressive. I feel like every intellect is pointed at one problem. Further, the support from people inside and outside of the hospital is truly overwhelming and much appreciated.
I have only glimpsed what this disease can do, so hats off to the leadership for their transparency and stewardship over the last 6 weeks. It is remarkable to witness the level of dedication of each individual trying to make a difference.
The Daily Beast: Here’s Where Coronavirus Hides in Your Body, by David Axe, 4/10/2020
“Active virus-replication in the upper respiratory tract puts the prospects of COVID-19 containment in perspective,” the scientists wrote.
Close observers of coronavirus studies hailed the German team’s work. There’s “huge news” in the Nature paper, David Ostrov, a professor in the Department of Pathology, Immunology and Laboratory Medicine at the University of Florida College of Medicine, told The Daily Beast.
SARS-CoV-2 starts replicating in the throat, not the lungs. For that reason, a simple throat swab is enough to test for the virus. There’s probably no need for an intrusive, unpleasant nasal swab.
There’s bad news in the German study, too.
The antibodies our bodies produce in response to COVID-19 infection don’t actually destroy this virus. In that way, it is a lot like HIV.
The antibodies are not effective at clearing the virus,” Ostrov told The Daily Beast. “This is relevant when thinking about viruses and vaccines. HIV also stimulates production of antibodies that fail to clear the virus, as do many other viruses, such as hepatitis virus C.”
“People have tried and failed to generate vaccines against such viruses, so we should not be overconfident that a vaccine strategy will work,” Ostrov added.
The Washington Post: I spent six days on a ventilator with covid-19. It saved me, but my life is not the same. By David Lat, 4/9/2020
I spent my first few days in the hospital in stable condition, receiving supplemental oxygen. But on the evening of March 20, I took a turn for the worse. Late that night, I learned that I would need to be intubated, or placed on a ventilator.
This terrified me. A few days earlier, after my admission to the hospital, my physician father had warned me: “You better not get put on a ventilator. People don’t come back from that.”
As a patient whose life was saved by a ventilator, I believe it is an outrage and an embarrassment that a nation as wealthy as ours is even discussing possible ventilator shortages. Thankfully the United States has managed to avoid widespread rationing partly due to ventilators being sent from places of low need to places of high need. We need to make sure that every patient who needs a ventilator can get one so that as many of them as possible can survive.
This is especially true because survival rates of ventilated patients are low. My father’s dark comment reflected a grim reality: 40 percent to 50 percent of patients with severe respiratory distress do not survive being on ventilators. In New York City, where I was hospitalized, 80 percent or more of coronavirus patients who end up on ventilators have died.
SciTechDaily: Possible Coronavirus Treatment? Head Lice Drug Ivermectin Is Being Tested, By Andrew McLachlan, the Head of School and Dean of Pharmacy, University of Sydney, Australia, 4/6/2020
SciTechDaily: Coronavirus Fight: Scientists Identify COVID-19 Drug That “Kills” the Virus Within 48 Hours, Wagstaff et al, 4/5/2020
Ivermectin is an FDA-approved anti-parasitic drug that has also been shown to be effective in vitro against a broad range of viruses including HIV, Dengue, Influenza and Zika virus.
While shown to be effective in the lab environment, Ivermectin cannot be used in humans for COVID-19 until further testing and clinical trials have been completed to confirm the effectiveness of the drug at levels safe for human dosing.
The wholesale cost in the developing world for the tablets is about US $0.12 for a course of treatment. In the United States, the costs is less than US$50.
So, the drug would be only 400x as expensive here, half of that plundered by Health Insurance Industrial Complex parasites.
Antiviral Research: The FDA-approved Drug Ivermectin inhibits the replication of SARS-CoV-2 in vitro, by Caly, Druce, Catton, Jans, & Wagstaff, 4/3/2020
AAPS Journal, The Pharmacokinetics and Interactions of Ivermectin in Humans—A Mini-review, by González Canga, A., et al, 1/25/2008
Although the efficacy of ivermectin has been established in humans against several parasite diseases, the pharmacokinetic properties of this compound are less well known in humans compared to animals. Potential drug-drug interactions and drug-food interactions exist for ivermectin, which should be considered during therapeutic use of this drug.
The New Yorker: The Quest for a Pandemic Pill, by Matthew Hutson, 4/6/2020
The New Yorker: How Does the Coronavirus Behave Inside a Patient?, by Siddhartha Mukherjee, 3/26/2020
Mukherjee's "The Emperor of All Maladies" won a Pulitzer Prize.
Los Angeles Times: Coronavirus kills some people and hardly affects others: How is that possible? by Deborah Netburn, 4/4/2020
CNN: Experts tell White House coronavirus can spread through talking or even just breathing, By Elizabeth Cohen,4/2/2020
Medium: NYC Lung Doctor Tells His Family How to Protect Themselves from COVID-19, by Paul Anderson, 3/27/2020
The New Yorker: From Bats to Human Lungs, the Evolution of a Coronavirus, by Carolyn Kormann, 3/27/2020
Since January, nearly eight hundred papers about the virus have been posted on BIORxiv, a preprint server for studies that have not yet been peer-reviewed. More than a thousand coronavirus genome sequences, from different cases around the world, have been shared in public databases. “It’s insane,” Kristian Andersen, a professor in the Department of Immunology and Microbiology at Scripps Research, told me. “Almost the entire scientific field is focussed on this virus now. We’re talking about a warlike situation.”
Medium: This Is How Your Immune System Reacts to Coronavirus, by Dana G Smith, 3/24/2020
Youtube: Ninja Nerd: Epidemics and the coronavirus infection, the ARDS and pneumonia timeline explained. 3/16/2020
Youtube: Ninja Nerd: COVID-19 | Corona Virus: Treatment, Prognosis, Precautions, 3/18/2020
Youtube: Duc C. Vuong, MD, explains how COVID-19 kills and why you can't be saved, 3/23/2020
CNN: Video reveals lung damage in US coronavirus patient: 'People need to take this seriously' By Brian Fung and Jen Christensen, 3/27/2020
University of Texas: COVID-19 Can Cause Cardiac Injury – Even in Patients Without Underlying Heart Conditions, University of Texas Health Science Center at Houston, 3/27/2020
In a clinical bulletin issued by the American College of Cardiology, it was revealed that the case fatality rate of COVID-19 for patients with cardiovascular disease was 10.5%. Data also points to a greater likelihood that individuals over the age of 65 with coronary heart disease or hypertension can contract the illness, as well experience more severe symptoms that will require critical care.
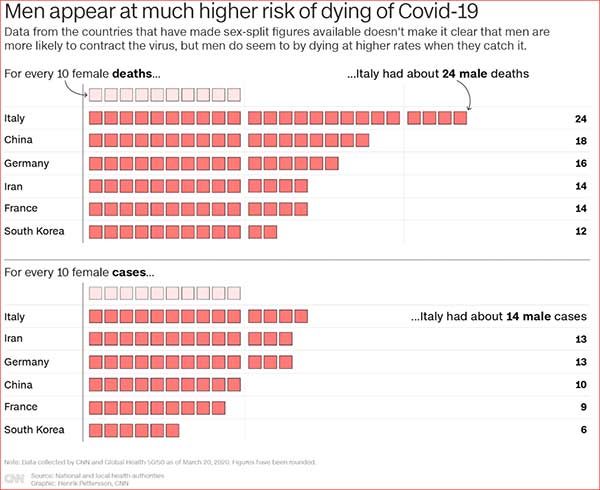
CNN: Here's why the coronavirus may be killing more men than women. The US should take note, By Katie Polglase, Gianluca Mezzofiore and Max Foster, 3/24/2020
Cell: Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein, Alexandra C. Walls, Young-Jun Park, M. Alejandra Tortorici, Abigail Wall, Andrew T. McGuire, David Veesler, 3/9/2020
Highlights
- SARS-CoV-2 uses ACE2 to enter target cells
- SARS-CoV-2 and SARS-CoV bind with similar affinities to ACE2
- Structures of SARS-CoV-2 spike glycoprotein in two conformations
- SARS-CoV polyclonal antibodies inhibit SARS-CoV-2 spike-mediated entry into cells
Time: About Dr. Frederick Murphy, the first CDC Virologist to image the Ebola Virus, Alexandra Sifferlin, 10/13/2014
Time: SARS, Ebola, Marburg, MERS infection rate and death tolls compared, David Johnson, 2014/10/13
Harvard Gazette: Samples from those who had COVID-19 could illuminate true infection rate, lethality, vaccines, Stephanie Dutchen, 3/25/2020
VirScan promises to help Elledge and colleagues identify which parts of the virus the immune system responds to.
Recent work from his group suggests that people all over world infected with a particular virus make antibodies against the same proteins — “even the same amino acids” — on that virus, Elledge said.
That’s surprising, considering how many epitopes viruses have and how many antibodies are in the body’s arsenal, said Elledge. The findings led him to suspect that some epitopes are, in effect, decoys, and therefore, that not all antibodies have the desired neutralizing effect.
“The immune system may be sending out all these antibodies like shooting a shotgun and hoping some of the spray will hit the target, neutralizing some critical part of the virus,” he said.
In principle, said Elledge, VirScan could indicate which epitopes are useful targets against the new coronavirus and which are just noise. Then researchers could eliminate the useless ones from vaccines they’re developing.
1918 Spanish Flu historical documentary | Swine Flu Pandemic | Deadly plague of 1918, 10/2/2018
Cambridge University: Spanish Flu: a warning from history, 11/30/2018
6/26/2017 Genomic Vaccines Fight Disease in Ways Not Possible Before, by Geoffrey Ling, Scientific American
Vaccines composed of DNA or RNA, instead of protein, could enable rapid development of preventives for infectious diseases